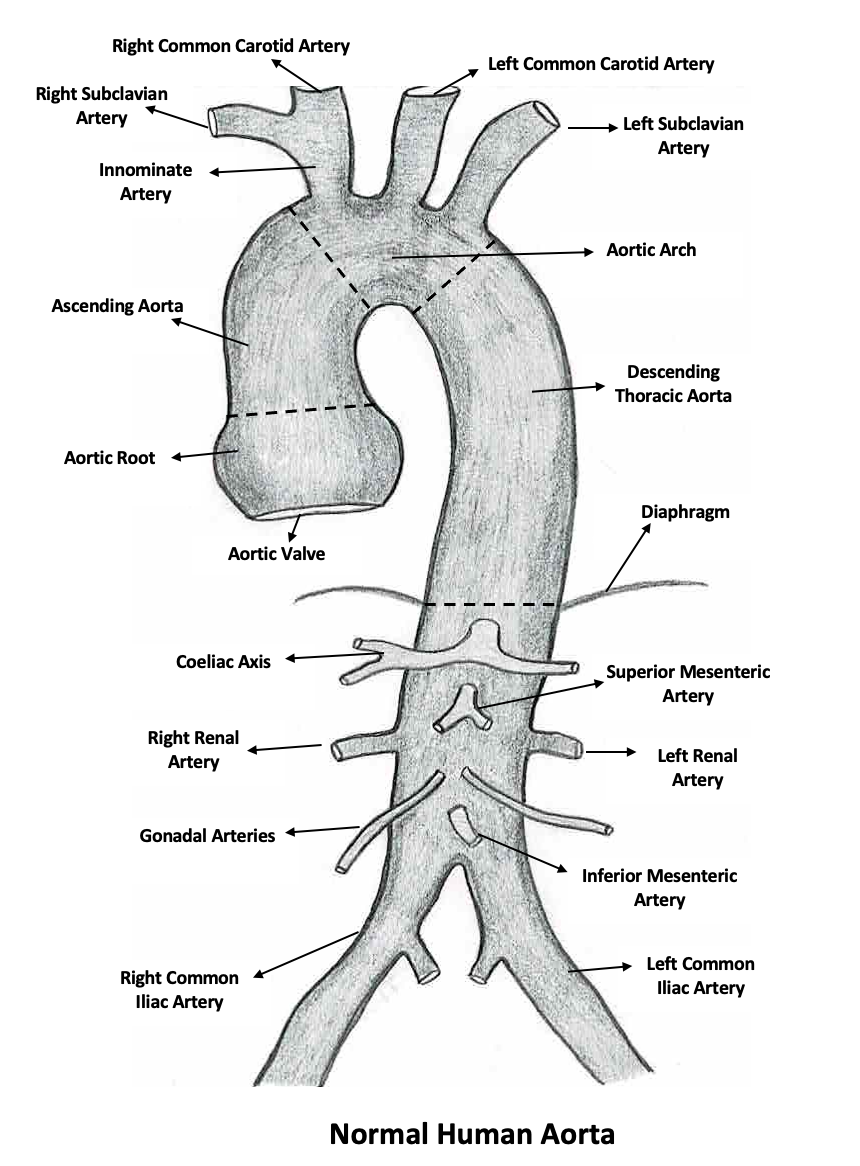
Aortic diseases encompass a range of conditions affecting the aorta (largest artery in the body), which arises from the heart and delivers oxygenated blood to the rest of the body. These diseases are significant due to the aorta's crucial role in the circulatory system and can be life-threatening if not diagnosed and treated promptly.
The most common aortic diseases include: Aortic aneurysms: An aortic aneurysm involves a dilation or bulging of a portion of the artery due to weakening of the artery wall. This can occur in any part of the aorta but is most common in the abdominal region. Risk factors for aneurysms include hypertension, high cholesterol, smoking, and genetic predispositions. A ruptured aortic aneurysm can lead to severe internal bleeding and is a medical emergency.
Aortic dissection: Aortic dissection is another critical condition where a tear in the inner layer of the aorta causes blood to flow between the layers of the wall of the aorta, forcing the layers apart. It is often characterized by sudden, severe pain in the chest or back. Risk factors are similar to those for aneurysms and include uncontrolled hypertension, connective tissue disorders like Marfan syndrome, and trauma. Immediate medical attention is vital for survival.
Treatments may include lifestyle modifications, medications to control blood pressure and cholesterol, and in severe cases, surgical interventions such as stent placement or aortic repair.
Early detection is crucial in managing aortic diseases. Regular check-ups and imaging tests like echocardiograms, CT scans, or MRI can help in early identification, especially for individuals at high risk. Advances in medical and surgical treatments have improved outcomes for many patients with aortic diseases, making timely diagnosis and intervention even more critical.
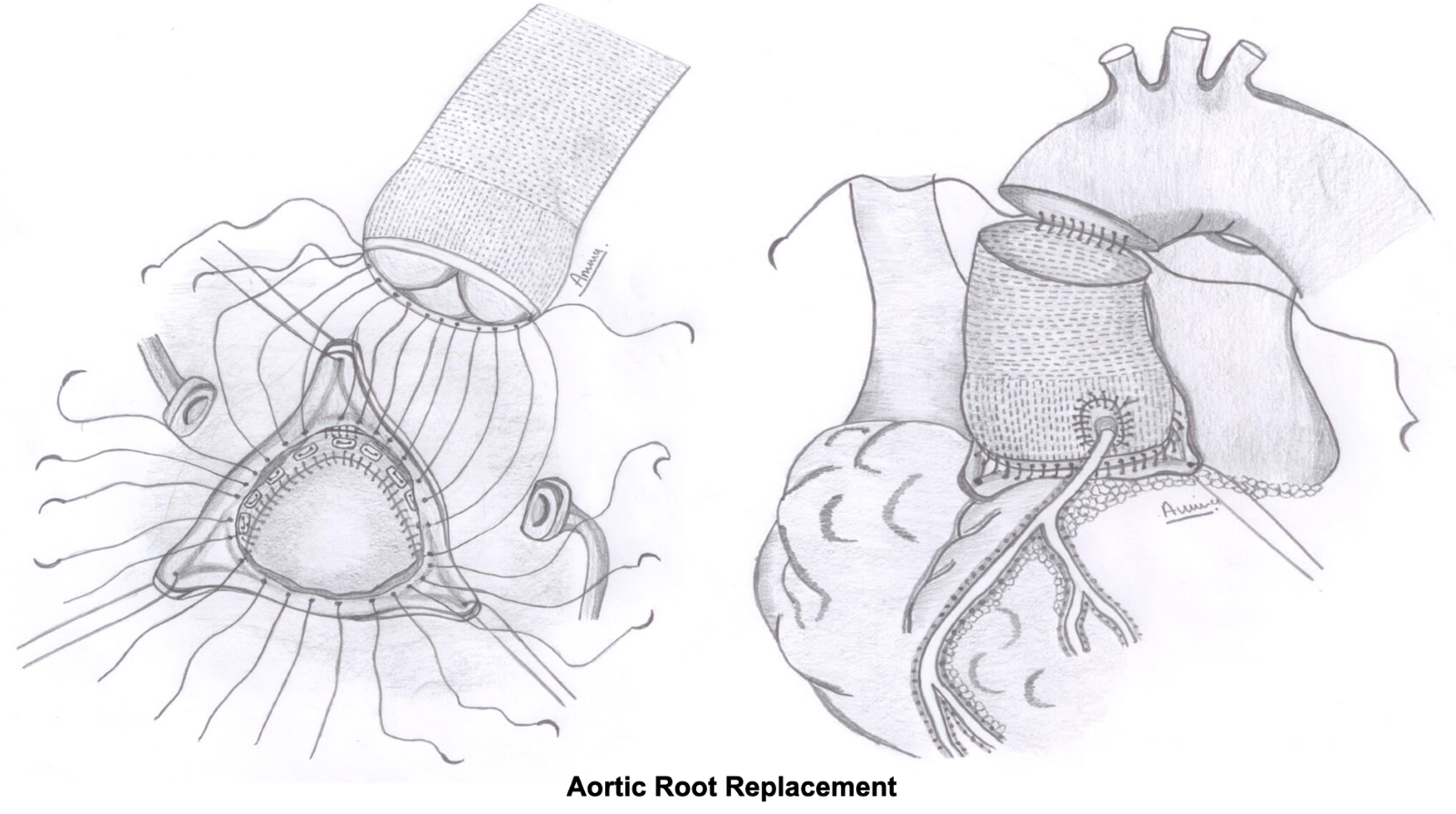
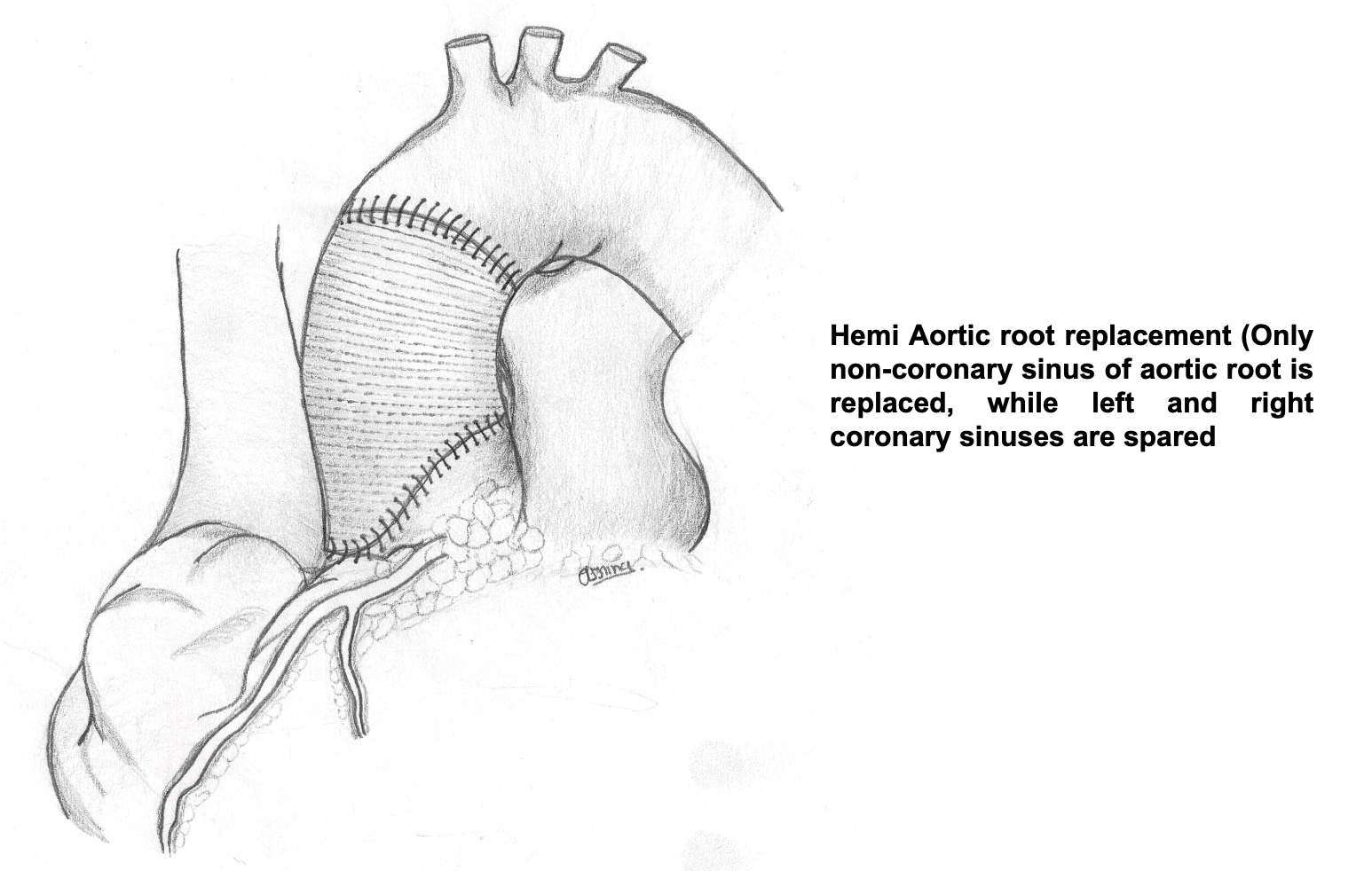
(i). Aortic Root Aneurysm Repair:
Aortic root enlargement involves the dilation/ enlargement of the aortic root, which is the segment of the aorta closest to the heart. This condition can be due to various causes, including genetic disorders like Marfan Syndrome, aortic valve disease, hypertension, and age-related changes. The aortic root plays a critical role in cardiovascular function, as it houses the aortic valve and is integral to the flow of blood from the heart to the rest of the body.
Surgical treatment for aortic root enlargement is considered when the risk of aortic rupture or dissection becomes significant, or if the patient is undergoing surgery for associated aortic valve disease. The main surgical procedures for this condition are:
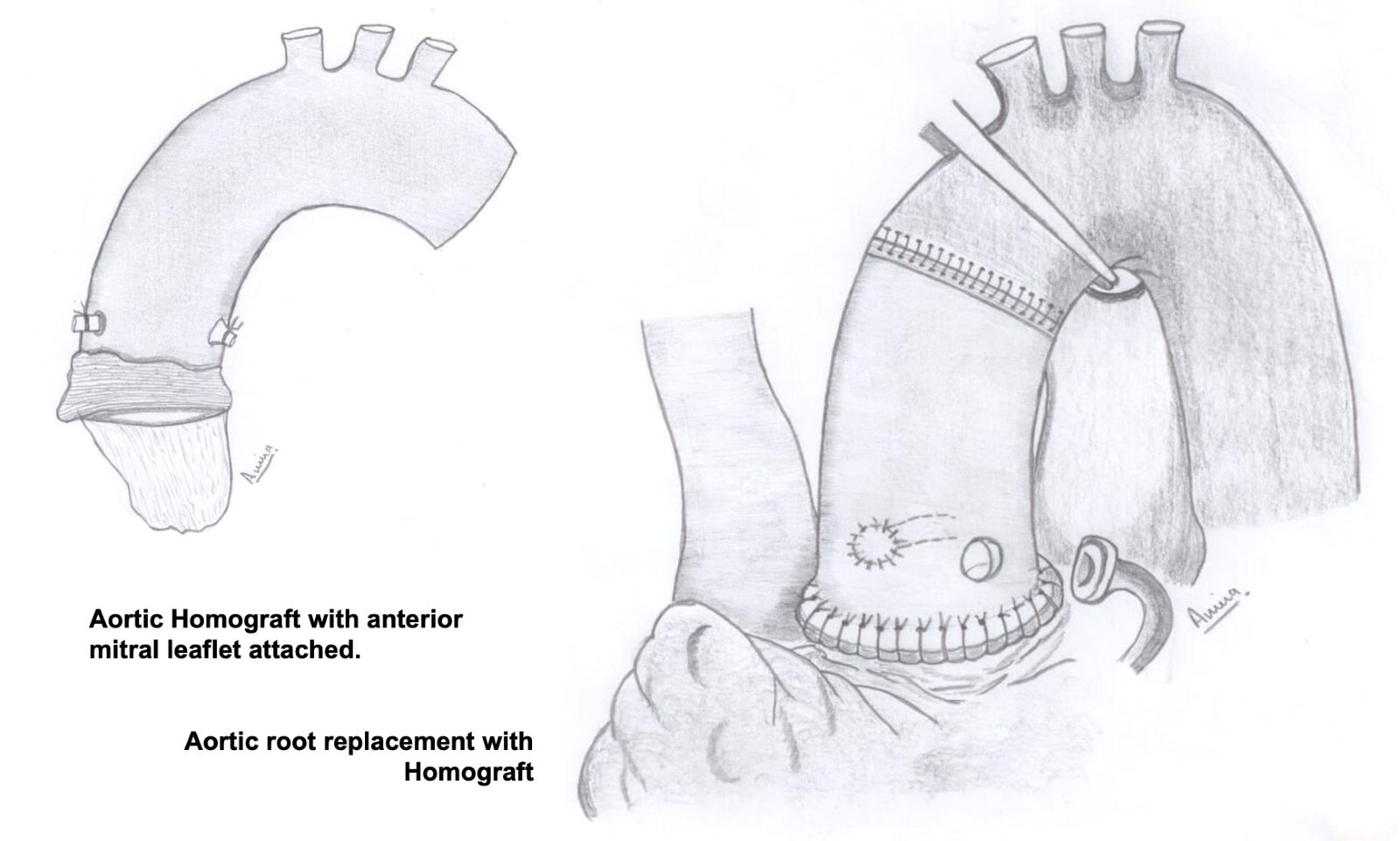
Aortic Root Replacement: This is the traditional approach and involves removing the enlarged section of the aorta and replacing it with a biological or synthetic graft. If the aortic valve is also diseased, it may be replaced with a mechanical or biological valve. This procedure is known as the Bentall procedure when it includes valve replacement.
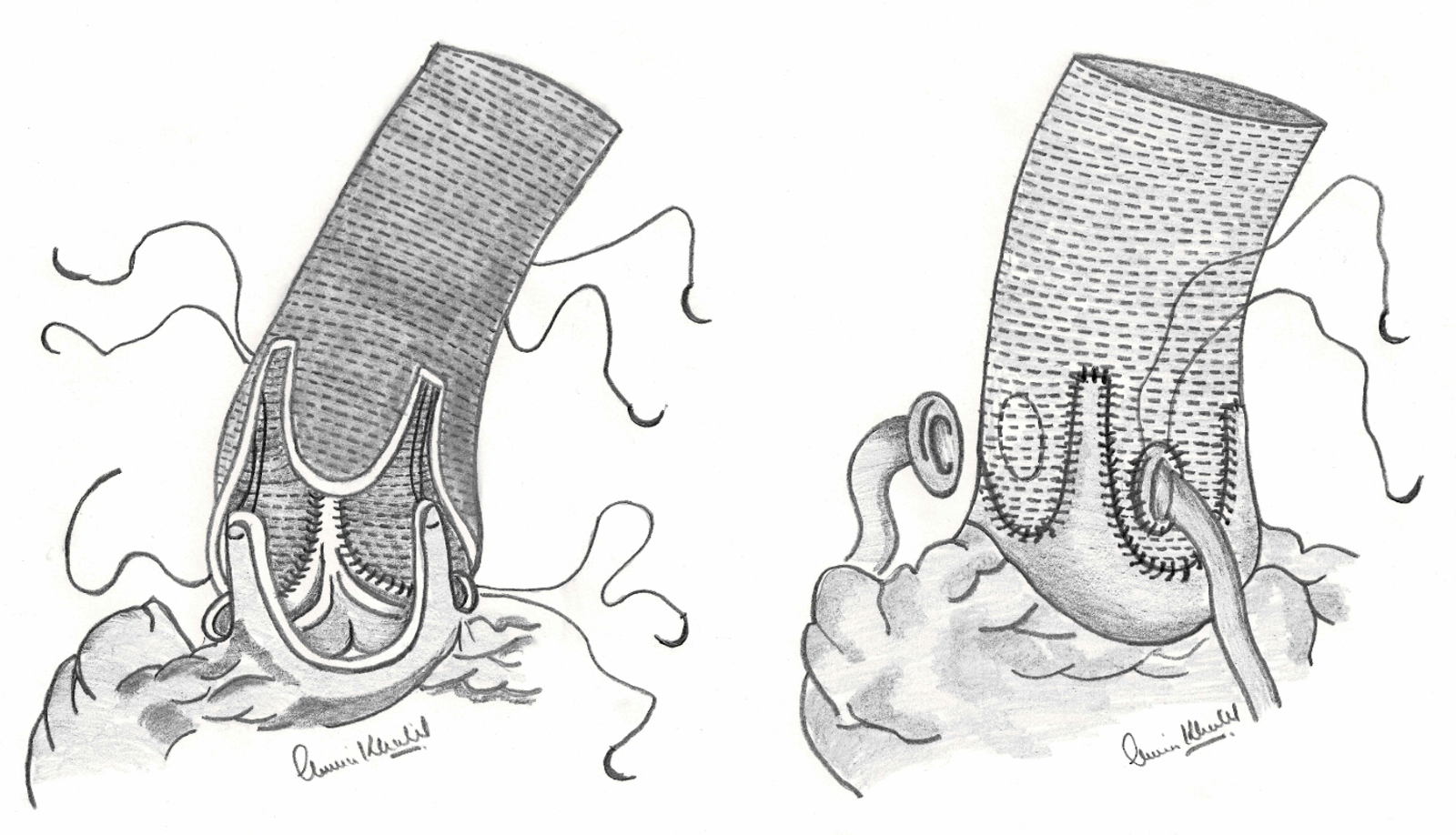
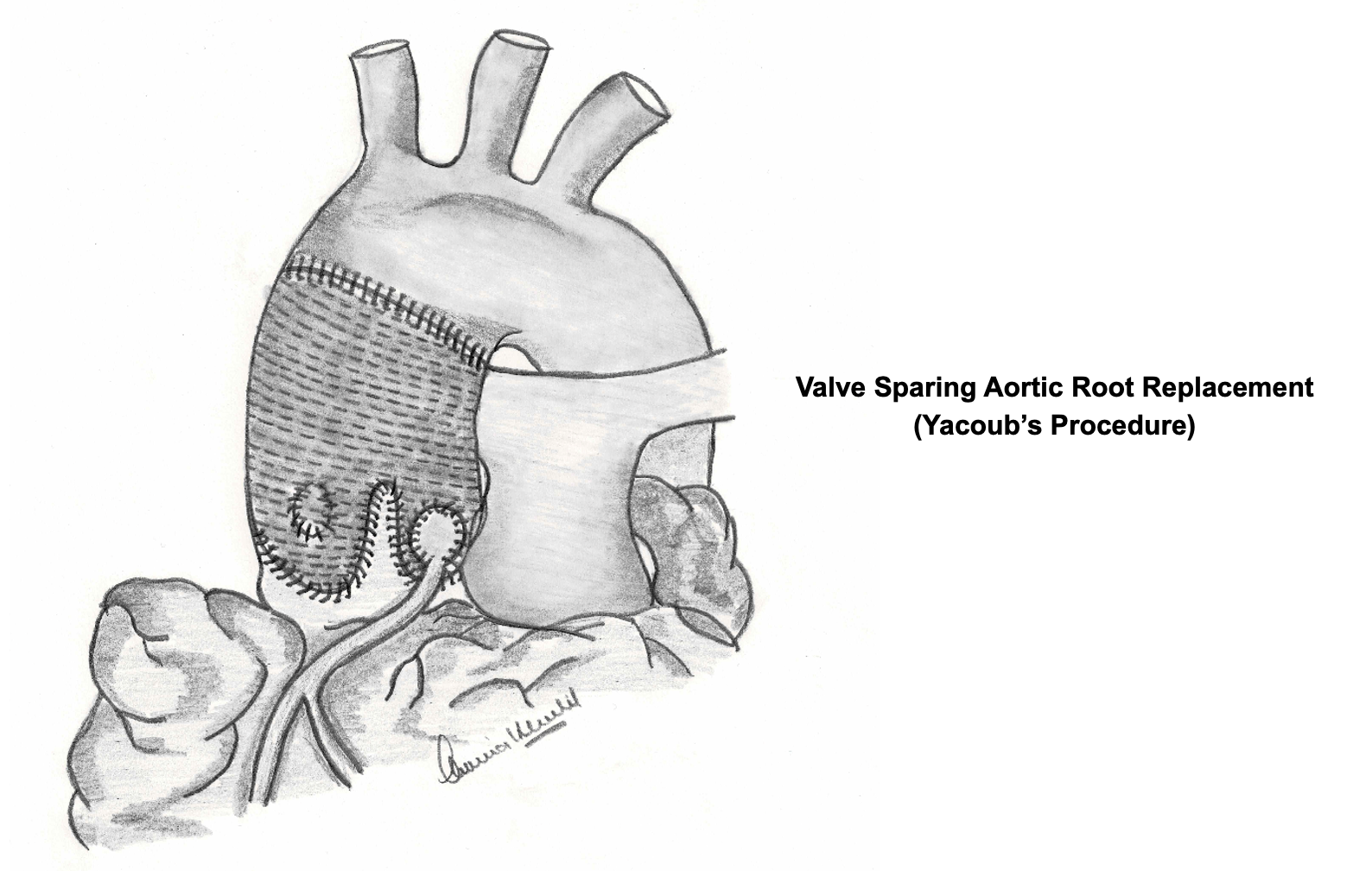
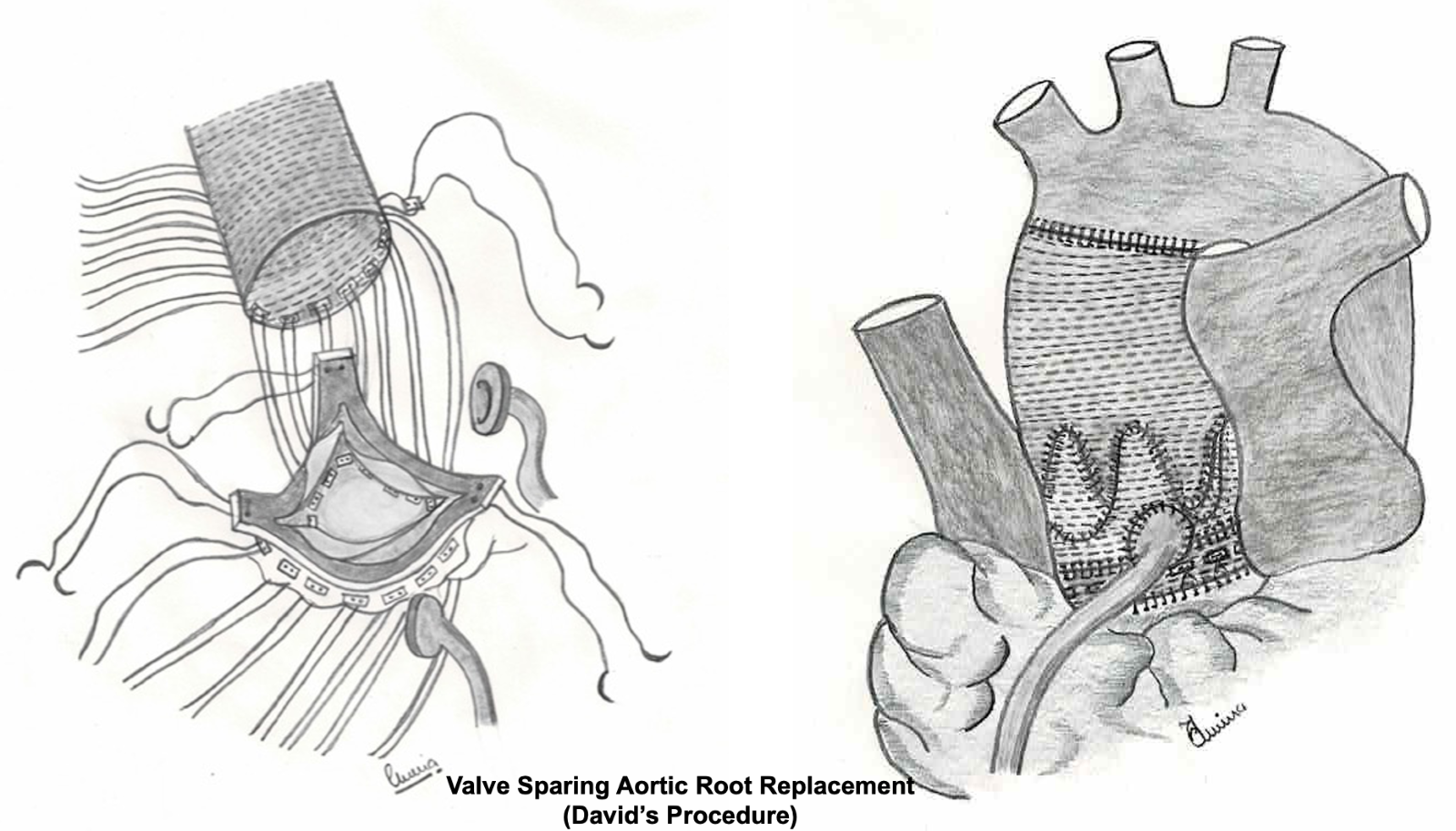
Valve-Sparing Aortic Root Replacement: In patients where the aortic valve is still functional, a valve-sparing procedure can be performed. This technique preserves the patient's native aortic valve while replacing the dilated aortic root with a graft. The two main types of valve-sparing procedures are the David and Yacoub techniques, which differ in how the aortic valve is preserved and re-implanted into the graft.
The choice of surgical procedure depends on several factors, including the patient's age, the condition of the aortic valve, the extent of aortic dilation, and the presence of any connective tissue disorders. These surgeries are complex and require a specialised team with high level of surgical expertise.
Postoperative care is crucial and includes regular monitoring of the aortic size and function, management of blood pressure, and lifestyle modifications to reduce the risk of future aortic complications. The long-term prognosis after aortic root surgery depends on the underlying cause of the enlargement, the patient's overall health, and the success of the surgery. Regular follow-ups with a cardiologist or a cardiovascular surgeon are essential to manage the condition effectively.
(ii). Ascending Aortic Replacement:
The replacement of the ascending aorta is a surgical procedure, performed to treat conditions such as aneurysms, dissections, or other diseases affecting this vital artery. The ascending aorta is a crucial part of the heart's anatomy, originating from the left ventricle and carrying oxygen-rich blood to the body.
The diseased/damaged segment of the artery is replaced using a synthetic tube, or graft. This procedure requires cardiopulmonary bypass, where a machine temporarily takes over the function of the heart and lungs during surgery. The complexity of the operation varies depending on the extent of the disease and the involvement of nearby structures, such as the aortic valve or the aortic arch.
Patients undergoing this surgery are carefully evaluated preoperatively to assess the risk and to plan the surgical approach. Regular follow-up and imaging studies are often necessary to monitor the graft and the overall condition of the cardiovascular system post-surgery.
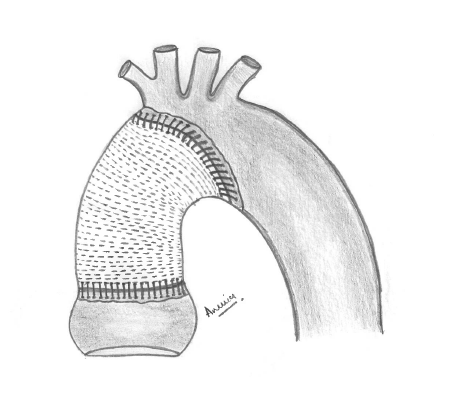
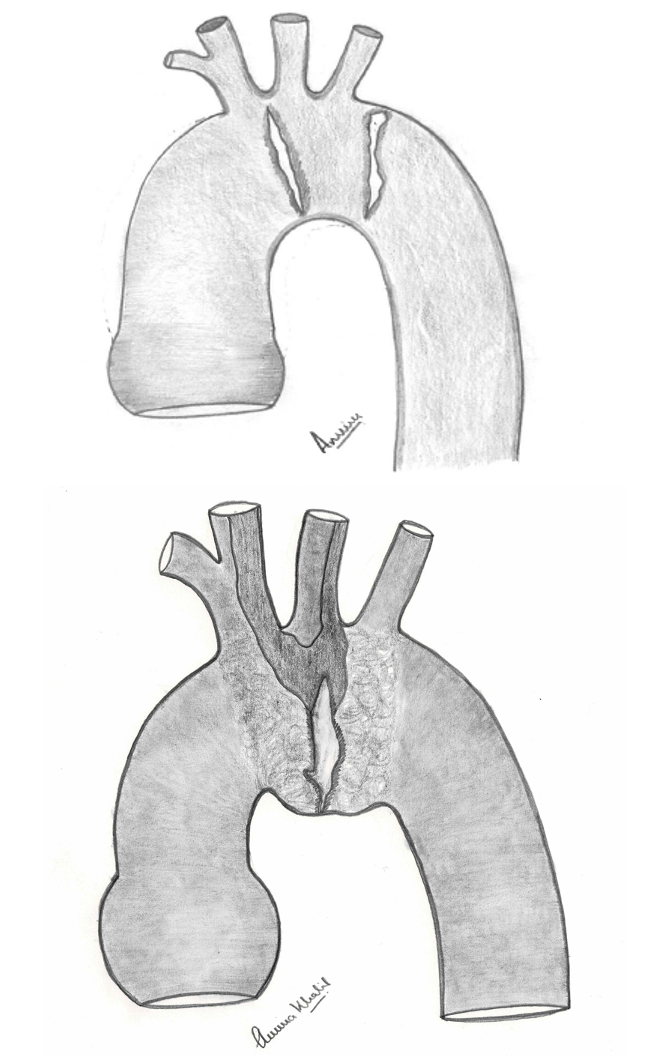
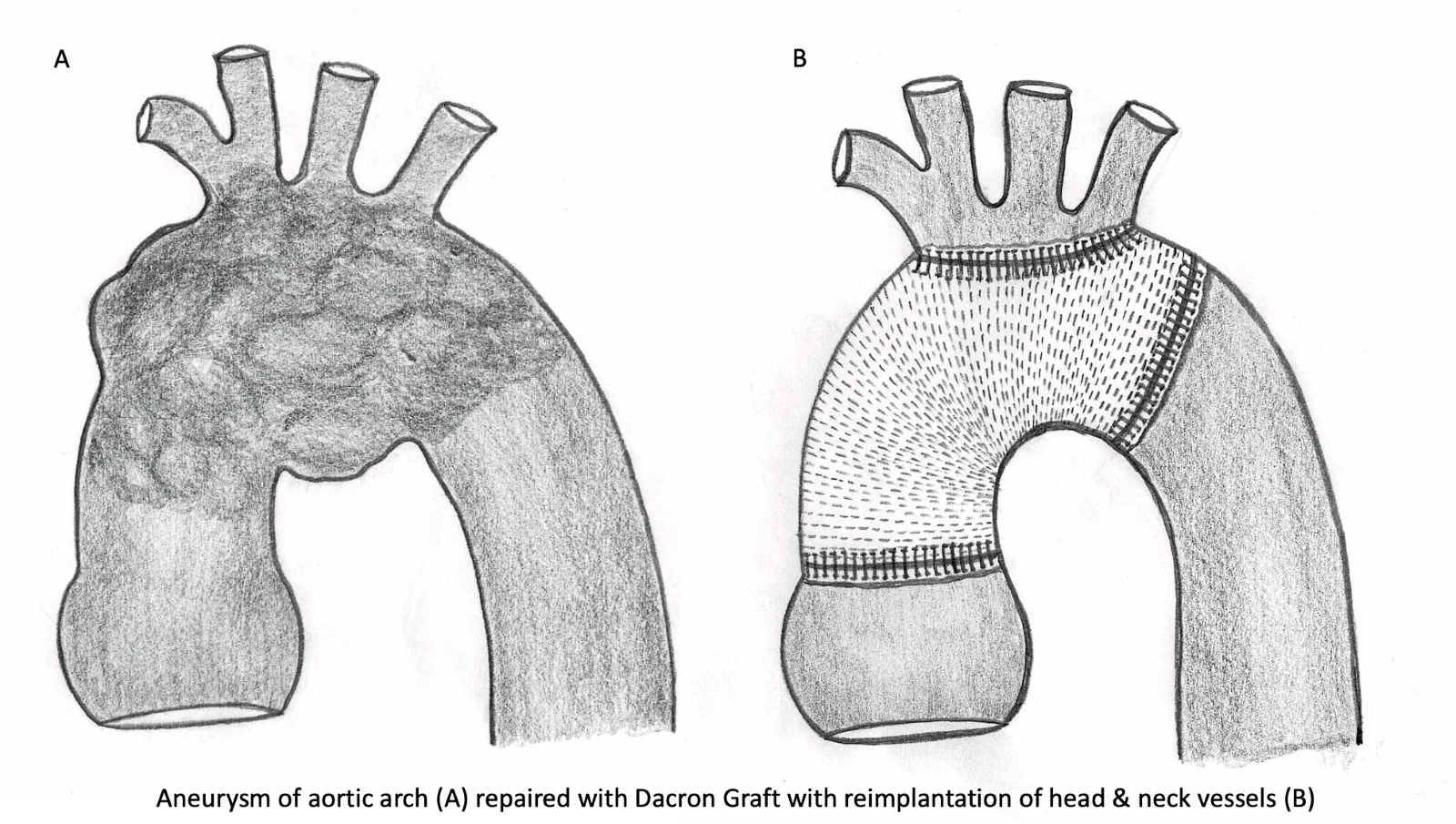
(iii). Aortic Arch Replacement:
The surgical treatment of aortic arch replacement is a complex and high-risk procedure, typically performed to address severe conditions affecting the aortic arch, such as aneurysms, dissections, or traumatic injuries. The aortic arch, a critical part of the cardiovascular system, is the section of the aorta that bends between the ascending and descending aorta, and any disease in this area requires expert medical intervention.
Aortic arch replacement involves replacing the diseased segment of the aortic arch with a synthetic graft. This is a major operation and requires the use of cardiopulmonary bypass (a heart-lung machine) and deep hypothermic circulatory arrest. The latter technique cools the patient's body to a very low temperature to protect the brain and other organs while blood flow is temporarily stopped to facilitate the replacement of the aortic segment.
One of the key challenges of aortic arch surgery is ensuring adequate protection of the brain during the period of circulatory arrest. Surgeons often employ advanced neuroprotective strategies, such as selective antegrade cerebral perfusion, where blood is delivered directly to the brain during the procedure.
Postoperative care is critical, with close monitoring for potential complications like stroke, bleeding, or infection. Recovery from such a major operation is often lengthy and requires a multidisciplinary team approach, involving cardiologists, cardiac surgeons, neurologists, and rehabilitation specialists.
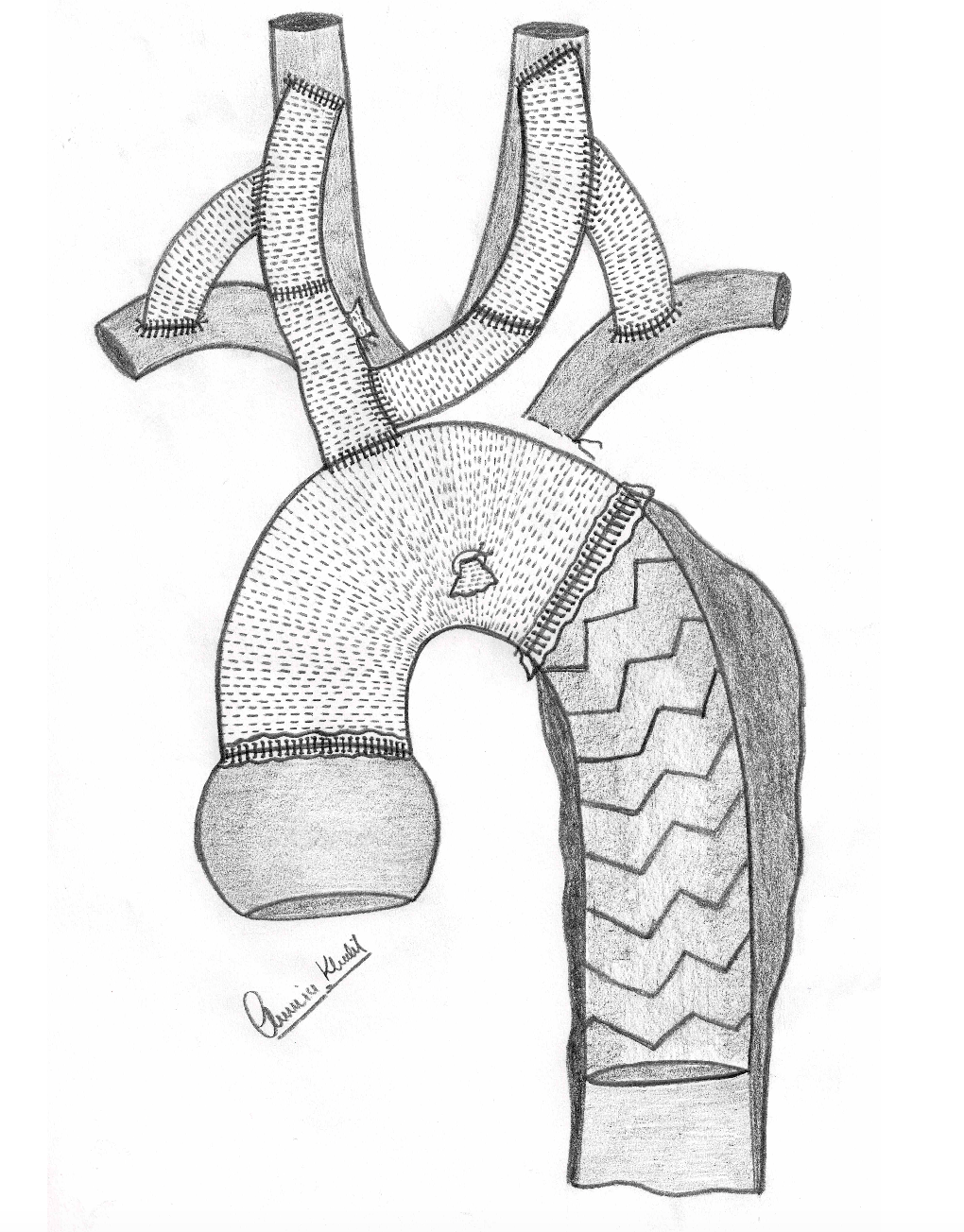
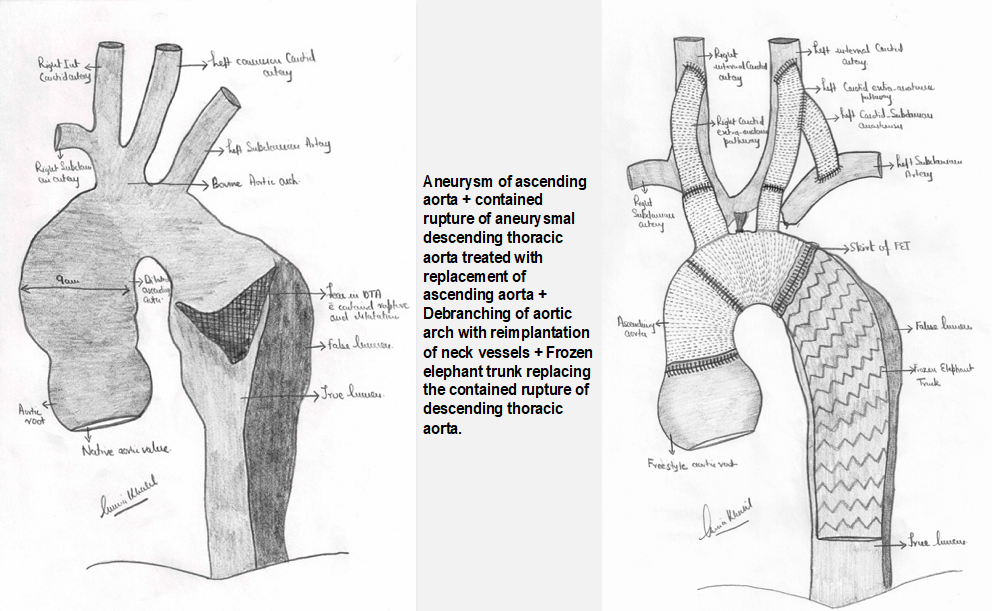
Frozen elephant trunk:
Aortic arch aneurysm/dissection extending to descending thoracic aorta, the head and neck vessels can be debranched and replaced with artificial conduits and can be connect to a specialised conduit /tube called as frozen elephant trunk.
Debranching of arch + TEVAR:
In a specific group of high-risk patients with significant comorbidities, the aortic arch can be debranched with reimplantation of head and neck vessels in ascending aorta. This creates a zone for deploying a stent for rest of disease artery. This stent deployment procedure is called as TEVAR.
(iv). Thoracoabdominal aneurysm repair:
Thoracoabdominal aneurysm (TAA) repair is a complex highly specialised procedure addressing aneurysms that span both the thoracic and abdominal aorta. These aneurysms present as abnormal bulges or ballooning due to weaknesses in the arterial wall. When these aneurysms extend from the chest (thoracic) into the abdomen (abdominal), it's referred to as a thoracoabdominal aneurysm. TAAs are less common than isolated abdominal aortic aneurysms but pose a higher risk due to their size and location. These aneurysms are particularly challenging due to their extensive nature and the vital organs and structures involved.
The goal of TAA repair is to prevent the aneurysm from rupturing, which can be life-threatening. This repair can be done through.
Open surgical repair involves a large incision, allowing the surgeon to directly access and replace the diseased section of the aorta with a synthetic graft. This approach is very effective, but is associated with some risks and relatively longer recovery period.
Endovascular repair a less invasive option, involves inserting a stent graft through a small incision in the groin. This stent graft reinforces the weakened aorta from the inside, reducing the risk of rupture. It's associated with a shorter hospital stay and quicker recovery, but not all patients are candidates for this approach.
Patients undergoing TAA repair undergo careful preoperative evaluation, including detailed imaging studies like echocardiogram, angiogram, CT scans or MRIs lung function tests to plan the procedure. Intraoperatively, skillful execution of planned operation with extensive monitoring is performed to minimise the risks and complications. Postoperatively, patients are monitored in intensive care units and require a period of rehabilitation. Long-term follow-up is necessary to monitor the graft and ensure the aneurysm does not recur.