Aortic valve disease is a condition affecting the aortic valve, one of the four valves in the heart. This valve plays a crucial role in controlling blood flow from the heart to the aorta, the main artery that distributes blood to the rest of the body. Aortic valve disease can manifest in two primary forms: aortic stenosis and aortic regurgitation.
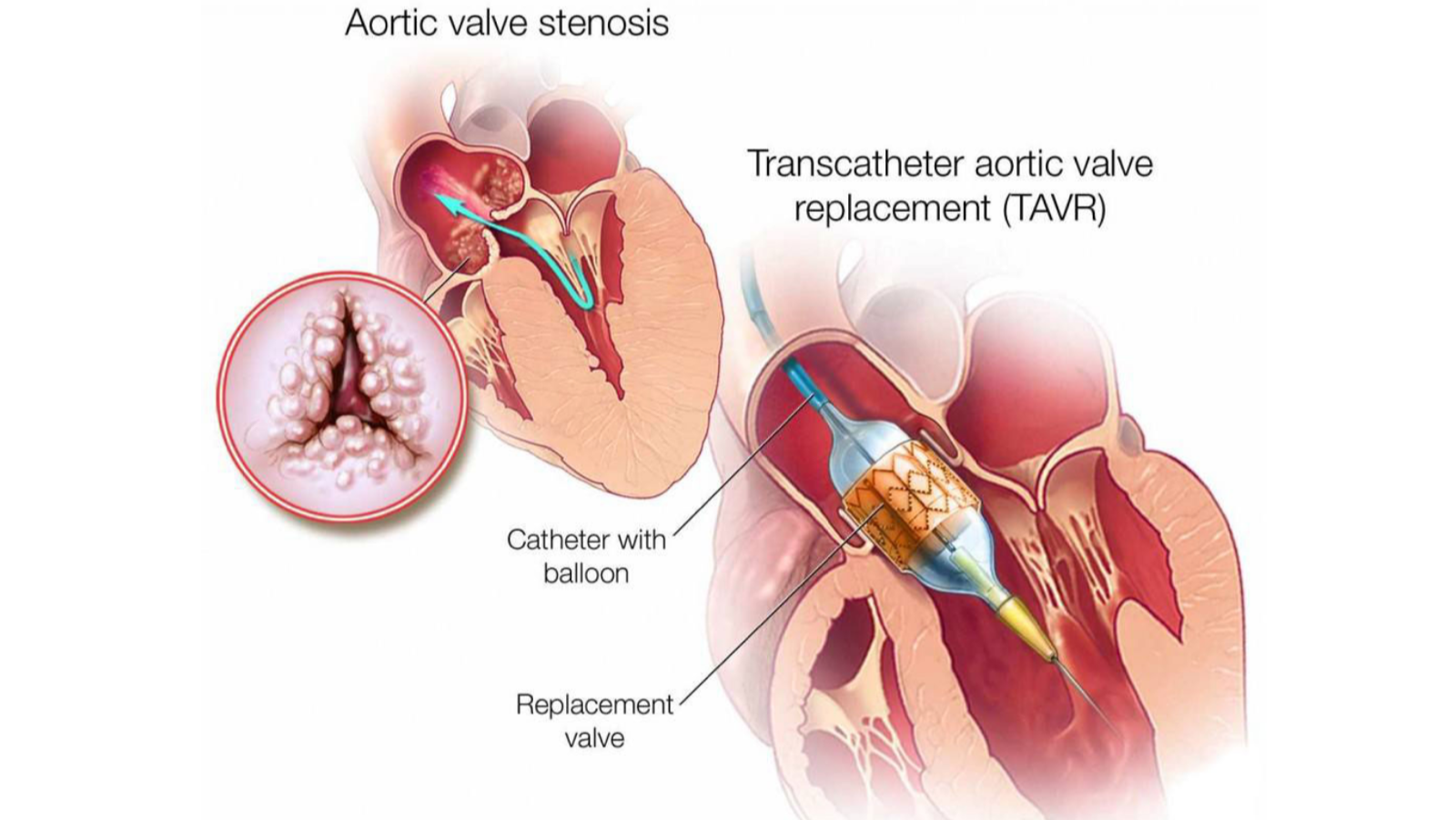
Aortic stenosis is characterised by the narrowing of the aortic valve. This narrowing hinders the valve from opening fully, which in turn reduces or obstructs blood flow from the heart to the aorta and onward to the rest of the body. The most common causes of aortic stenosis include age-related calcification of the valve, congenital valve abnormalities (like a bicuspid aortic valve), and rheumatic fever, which can damage the valve. Symptoms of aortic stenosis can include chest pain, fainting, fatigue, shortness of breath, and heart palpitations. The condition can lead to serious complications like heart failure, stroke, and blood clots if left untreated.
Aortic regurgitation on the other hand, occurs when the aortic valve does not close properly, leading to the backflow of blood from the aorta into the left ventricle. This condition can result from various factors, including valve deterioration due to aging, endocarditis (infection of the valve), high blood pressure, or connective tissue diseases. Symptoms of aortic regurgitation may include fatigue, shortness of breath, swelling of the ankles and feet, and palpitations. If severe and untreated, it can lead to heart failure and other critical complications.
Surgical intervention is necessary for severe cases, and the two primary options are Aortic Valve Replacement (AVR) and Transcatheter Aortic Valve Replacement (TAVR).
Cardicure offers all three choices of surgical aortic valve replacement:
Aortic valve replacement with Median sternotomy
Minimally invasive aortic valve replacement
Transcatheter aortic valve replacement
(i). Aortic Valve Replacement (AVR):
Conventional Aortic Valve Replacement (AVR) is a surgical procedure primarily aimed at treating aortic valve disorders such as aortic stenosis or aortic regurgitation. This procedure involves resecting the diseased valve replacing the malfunctioning valve with a prosthetic one.
The replacement valves are of two types:
1. Mechanical valves, made from durable materials requiring lifelong anticoagulation therapy,
2. Biological valves, made from animal tissue or human donor tissue, which may require replacement after several years but do not necessitate long-term anticoagulation.
The surgical process commences with general anesthesia and is followed by a median sternotomy, where a vertical incision is made down the middle of the chest to access the heart. Cardiopulmonary bypass (CPB) is essential for this surgery, as it takes over the function of the heart and lungs during the operation, allowing the heart to be stopped and giving the surgeon a motionless and bloodless field to work.
Once the heart is stopped, the surgeon opens the aorta, the main artery coming from the heart, to access the aortic valve. The diseased valve is carefully excised, and precise measurements are taken to ensure the appropriate size of the prosthetic valve. The new valve is then sutured into place. This process requires meticulous attention to detail, as proper placement and secure suturing are critical for the function of the new valve and the prevention of complications such as paravalvular leak. After the new valve is in place, the aorta is closed, and the heart is restarted. The patient is gradually weaned off the cardiopulmonary bypass machine. The sternotomy is then closed using wires to bring together the sternum, and the overlying tissue and skin are sutured.
Postoperative care is crucial and includes monitoring for complications such as bleeding, infection, and proper function of the new valve. Anticoagulation therapy is often required, especially with mechanical valves, to prevent blood clots.
Conventional AVR remains a gold standard treatment for severe aortic valve disease. It is a highly effective treatment with a good track record of significant symptom relief, improving life expectancy and quality of life with acceptable minimal risk. Since, it is an invasive procedure with associated risks, hence careful patient selection and skilled surgical execution are paramount.
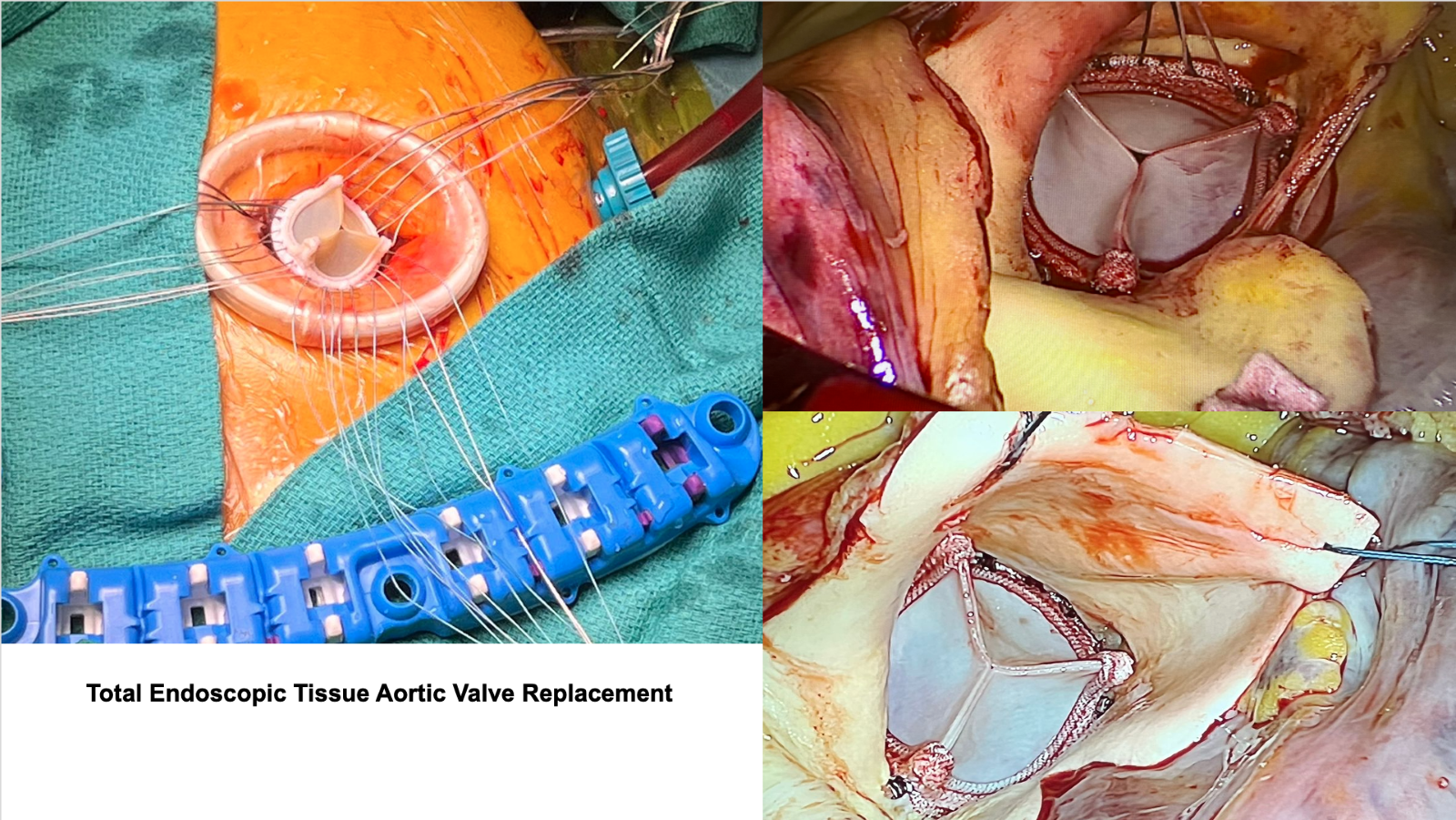
Minimally Invasive Aortic Valve Replacement (MIAVR) represents a significant advancement in cardiac surgery, and offers a less intrusive alternative to conventional open-heart surgery for aortic valve disorders. This procedure primarily targets the aortic valve, often affected by conditions such as aortic stenosis or regurgitation.
The surgical aspect of MIAVR is distinguished by smaller incision size which significantly reduces trauma, leading to relatively shorter hospital stays, less pain, and faster recovery times for patients. In MIAVR, the surgeon operates through these smaller openings using specialized instruments. The damaged valve is accessed and replaced with a prosthetic valve. The choice of the prosthetic valve – mechanical or biological – depends on various patient-specific factors, such as age, lifestyle, and medical condition. The precision required in MIAVR is facilitated by advanced imaging techniques, such as echocardiography, 3D monitors, which guide the surgeon throughout the procedure.
Comparable to conventional aortic valve replacement, MIAVR uses cardiopulmonary bypass, a machine that temporarily takes over the function of the heart and lungs during the surgery. This allows the surgeon to operate on a still, bloodless heart.
The evolution of MIAVR reflects a broader trend in surgery towards procedures that minimise physical trauma and expedite patient recovery. It demands high surgical skill and expertise, and its success rates have been comparable to traditional methods, making it a viable option for many patients requiring aortic valve replacement.
A less invasive alternative to AVR, TAVR is preferred for patients at intermediate or high risk for open-heart surgery. This procedure involves inserting a catheter, usually through the femoral artery in the groin, and guiding it to the heart. A collapsed replacement valve is then expanded at the site of the old valve. TAVR has a shorter recovery time and is associated with lower immediate procedural risk compared to AVR. However, it may not be suitable for all patients, especially those with certain anatomical considerations or other heart conditions.
Patient selection for either procedure depends on various factors, including age, physical health, the severity of stenosis, and the presence of other medical conditions. Regular follow-ups and echocardiographic evaluations post-surgery are essential to monitor valve function and ensure ongoing cardiac health.
2. Mitral Valve Disease:
Mitral valve is a left sided inlet valve which plays a crucial role in ensuring proper blood flow from the left atrium to the left ventricle. Mitral valve disease is a complex condition requiring careful management to prevent long-term complications and maintain quality of life. Mitral valve disease manifests in two main forms:
Mitral regurgitation is the most common form, where the valve doesn't close tightly, causing blood to flow backward into the left atrium. This backward flow forces the heart to work harder to pump sufficient blood, leading to symptoms like shortness of breath, fatigue, and, in severe cases, heart failure. The causes of regurgitation vary, including mitral valve prolapse (where valve flaps bulge into the atrium), rheumatic heart disease, infective endocarditis, or degenerative changes related to aging.
Mitral stenosis, on the other hand, is characterized by a narrowing of the mitral valve, impeding blood flow between the left atrium and ventricle. This narrowing usually results from scarring caused by rheumatic fever, a complication of strep throat that is now rare in developed countries. Patients with stenosis often experience symptoms like shortness of breath, especially during physical exertion, palpitations, and fatigue.
Treatment options vary depending on the severity and type of the disease. Medications like diuretics, beta-blockers, or anticoagulants are commonly prescribed to manage symptoms and prevent complications in early stages of disease. In more severe cases, surgical interventions such as valve repair or replacement is commanded. Surgical intervention can be performed with
Mitral valve repair/replacement with median sternotomy
Minimally invasive Mitral valve repair/replacement.
Transcatheter mitral valve replacement.
Mitra clip placement
(i). Mitral Valve Repair/Replacement (MVR):
Surgical intervention for mitral valve disorders, encompassing both repair and replacement, is a critical aspect of treating cardiac conditions. Mitral valve repair is often preferred over replacement due to its advantages in preserving the patient's native valve structure, which is beneficial for maintaining the normal heart function and reducing the need for lifelong anticoagulation therapy.
Surgical techniques employed for mitral valve repair, vary based on the pathology of the valve. Techniques such as resection or plication of the leaflets, chordal shortening or transfer, and annuloplasty (where a ring is implanted to reinforce the annulus) are common. The goal is to restore proper leaflet coaptation and valve competence while preserving as much of the native valve tissue as possible. This approach is associated with lower morbidity and mortality, better postoperative ventricular function, and a reduced risk of prosthesis-related complications.
When repair is not feasible, mitral valve replacement is performed. This involves removing the diseased valve and replacing it with a mechanical or bioprosthetic valve. Mechanical valves are durable but require lifelong anticoagulation to prevent thrombosis. Bioprosthetic valves, made from animal tissues, have a limited lifespan but often don't necessitate long-term anticoagulation. The choice between these prostheses depends on various factors, including patient age, comorbidities, and lifestyle.
The surgical approach is guided by the patient's overall condition and plays a crucial role in the outcome. Postoperative care is vital, with close monitoring for complications such as arrhythmias, heart failure, or valve dysfunction. Regular follow-up and echocardiographic evaluation are essential to assess valve function and ensure patient well-being.
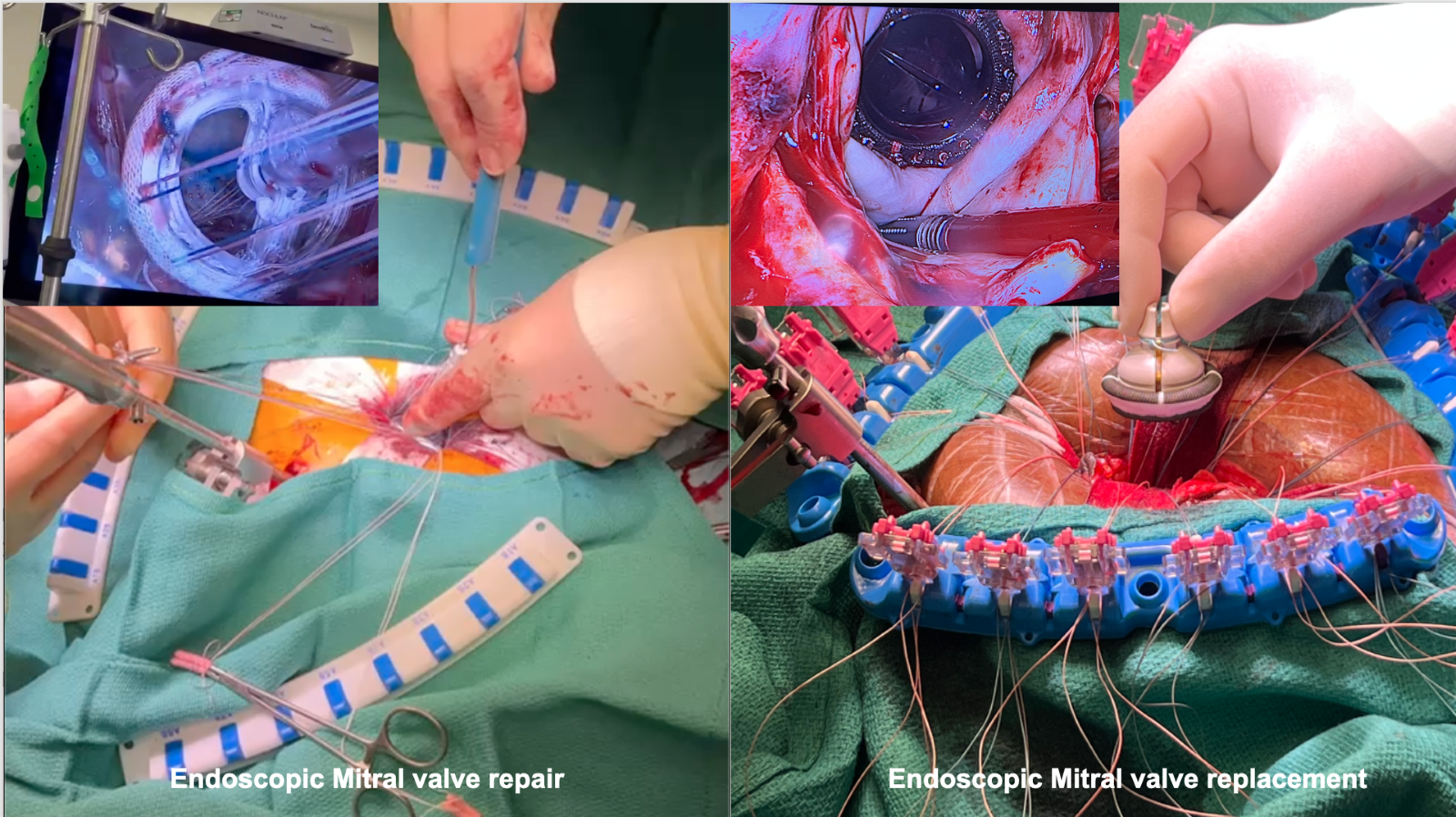
Minimally invasive mitral valve repair and replacement represent a significant advancement in cardiac surgery, emphasizing smaller incisions, reduced trauma, and quicker recovery times compared to traditional open-heart surgery. This approach involves accessing the mitral valve through a small incision, made in the right side of the chest, bypassing the need to open the entire chest cavity.
The procedure is conducted using specialised instruments and 3D cameras, allowing for greater precision and control. This technology enhances the surgeon's dexterity and visualisation, facilitating complex manoeuvres in a confined space. One of the key benefits is the direct and clear view of the mitral valve, which is crucial for precise repair or replacement.
When possible mitral valve repair is preferred over replacement, as it preserves the patient's own valve and offers better long-term outcomes. Techniques such as resection or artificial chordae implantation are used to correct the underlying issues causing mitral regurgitation. In cases where repair is not feasible, a prosthetic valve is used for replacement.
Postoperative recovery is significantly improved with this minimally invasive approach. Patients typically experience less pain, lower risk of infection, and faster return to normal activities. Moreover, the smaller incision leads to better cosmetic outcomes, an aspect important to many patients.
However, not all patients are candidates for this procedure. The decision depends on the patient's overall health, the condition of the mitral valve, and the presence of other cardiac or health issues. Our surgical team, including the cardiologist and cardiac surgeon, will thoroughly evaluate each case to determine the best approach.
(iii). Transcatheter mitral valve replacement:
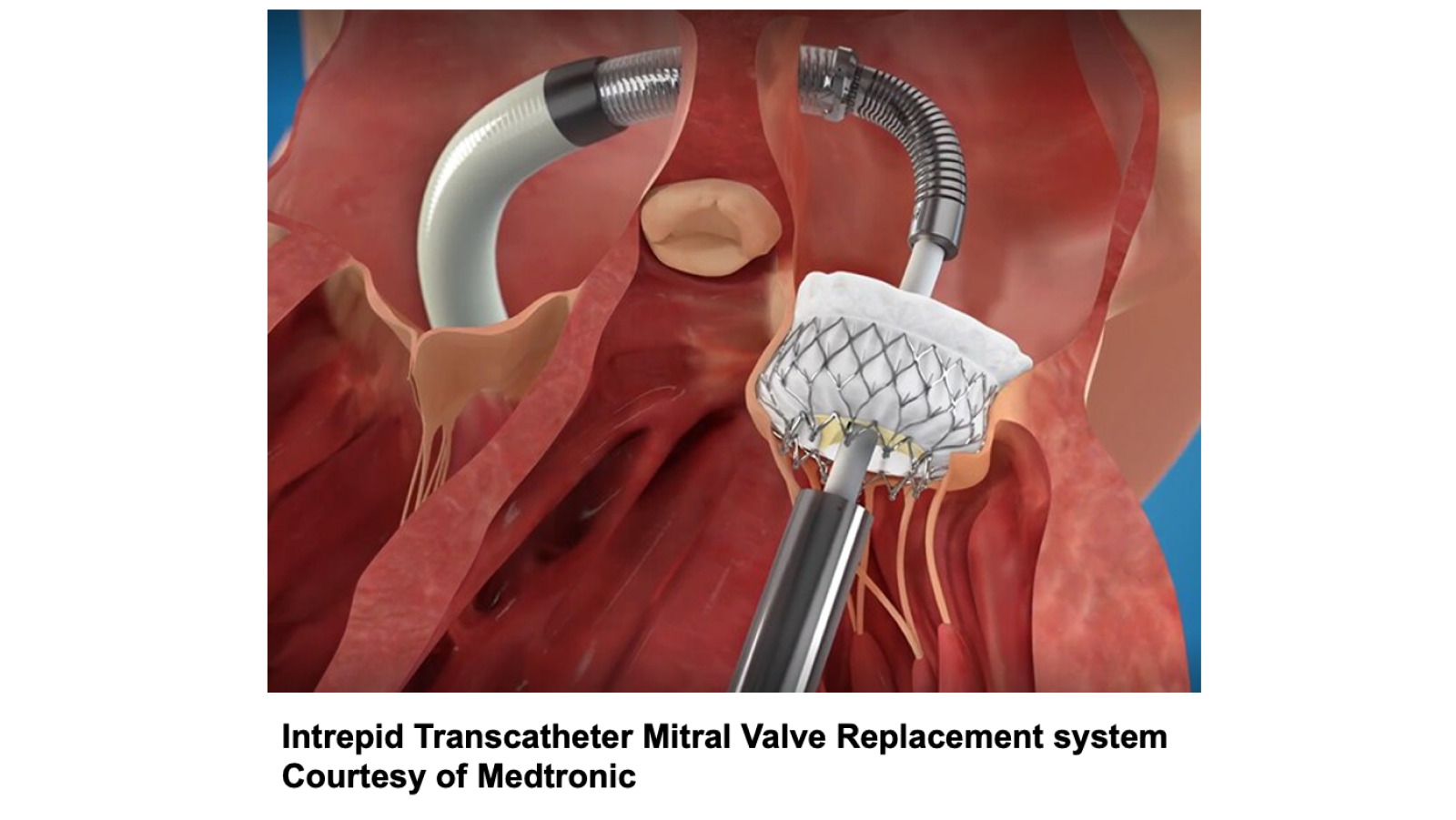
Transcatheter Mitral Valve Replacement (TMVR) is an innovative surgical procedure, particularly for patients deemed high-risk for conventional surgery. This minimally invasive technique involves the replacement of the mitral valve through a catheter, typically inserted via the femoral vein, avoiding the need for open-heart surgery and its associated risks.
The procedure starts with a small incision in the groin, through which the catheter is inserted and carefully guided to the heart using advanced imaging techniques. This precision is crucial, as the mitral valve has a complex anatomy and is located in a challenging position within the heart. Once in place, the new valve, often made of bioprosthetic material, is expanded and deployed, replacing the dysfunctional native valve.
TMVR offers several advantages over traditional surgery. It significantly reduces recovery time and hospital stay, lowers the risk of infection, and is less taxing on the patient's body, making it a viable option for older or frail patients. Moreover, the procedure can be performed under conscious sedation, avoiding the risks associated with general anesthesia.
However, TMVR is not without challenges. Precise placement of the valve is critical to avoid complications like valve leakage or obstruction of blood flow. The procedure also requires exceptional coordination among a multidisciplinary team, including cardiologists, cardiac surgeons, and imaging specialists.
(iv). Mitra Clip Placement:
The MitraClip procedure is a significant advancement in minimally invasive surgical technique designed to treat mitral valve regurgitation, offering a safer and less invasive option for treating mitral valve regurgitation, especially beneficial for high-risk patients. Its innovative approach, combined with the use of sophisticated imaging techniques, has made it a valuable tool for cardiac interventions This innovative procedure provides a vital alternative for patients who are deemed high-risk for conventional open-heart surgery.
The essence of the MitraClip technique lies in its minimal invasiveness. It involves a small incision in the femoral vein, through which a catheter is guided to the heart. Using advanced imaging techniques, the catheter is precisely navigated to the mitral valve. Here, the MitraClip device is deployed to clip the mitral valve leaflets together. This clipping action effectively reduces the gap in the mitral valve, thus minimizing the backflow of blood into the left atrium.
One of the significant advantages of the MitraClip procedure is the reduced recovery time compared to traditional surgery. Patients usually experience a quicker return to normal activities, and the risks associated with open-heart surgery, such as infection and prolonged recovery, are significantly lessened.
The procedure's precision is bolstered by the use of real-time transoesophageal echocardiography, which provides detailed images of the heart's structures. This allows for precise placement of the clip and immediate assessment of the procedure's effectiveness.
However, it's important to note that the MitraClip procedure may not be suitable for all patients with mitral valve regurgitation. The decision to use this technique is based on a variety of factors, including the severity and cause of the valve leakage, the patient's overall health, and the structure of their heart. The procedure's success also hinges on the expertise of the multidisciplinary team, including interventional cardiologists and cardiac surgeons, who collaborate to ensure the optimal outcome for each patient.
3. Tricuspid Valve Disease:
Tricuspid valve is a right sided inlet valve between right atrium and the right ventricle. It controls the flow of blood from the upper to the lower right chambers of the heart. Tricuspid valve disease is a less common than diseases of the left heart valve. The disease can manifest in two primary forms:
Tricuspid Stenosis: This condition results from narrowing of tricuspid valve, obstructing blood flow from the right atrium to the right ventricle. The most common cause of tricuspid stenosis is rheumatic heart disease, although it can also result from congenital defects or carcinoid syndrome. Patients with tricuspid stenosis often experience symptoms like fatigue, swelling in the abdomen or legs, and pulsations in the neck. The reduced blood flow can lead to congestion in the liver and other organs.
Tricuspid Regurgitation: In this form of the disease, the tricuspid valve fails to close properly, allowing blood to flow backward into the right atrium when the right ventricle contracts. This condition is caused by right ventricular dilation, endocarditis, or rheumatic heart disease, as well as trauma. Symptoms of tricuspid regurgitation often mirror those of heart failure and may include fatigue, swollen abdomen or legs, and liver congestion.
The specific symptoms and severity of the condition guide the treatment approach. Mild cases may only require monitoring, while more severe cases refractory to medical management could necessitate medication, such as diuretics to manage fluid retention or surgery intervention. The surgical intervention includes:
Tricuspid valve repair
Tricuspid valve replacement
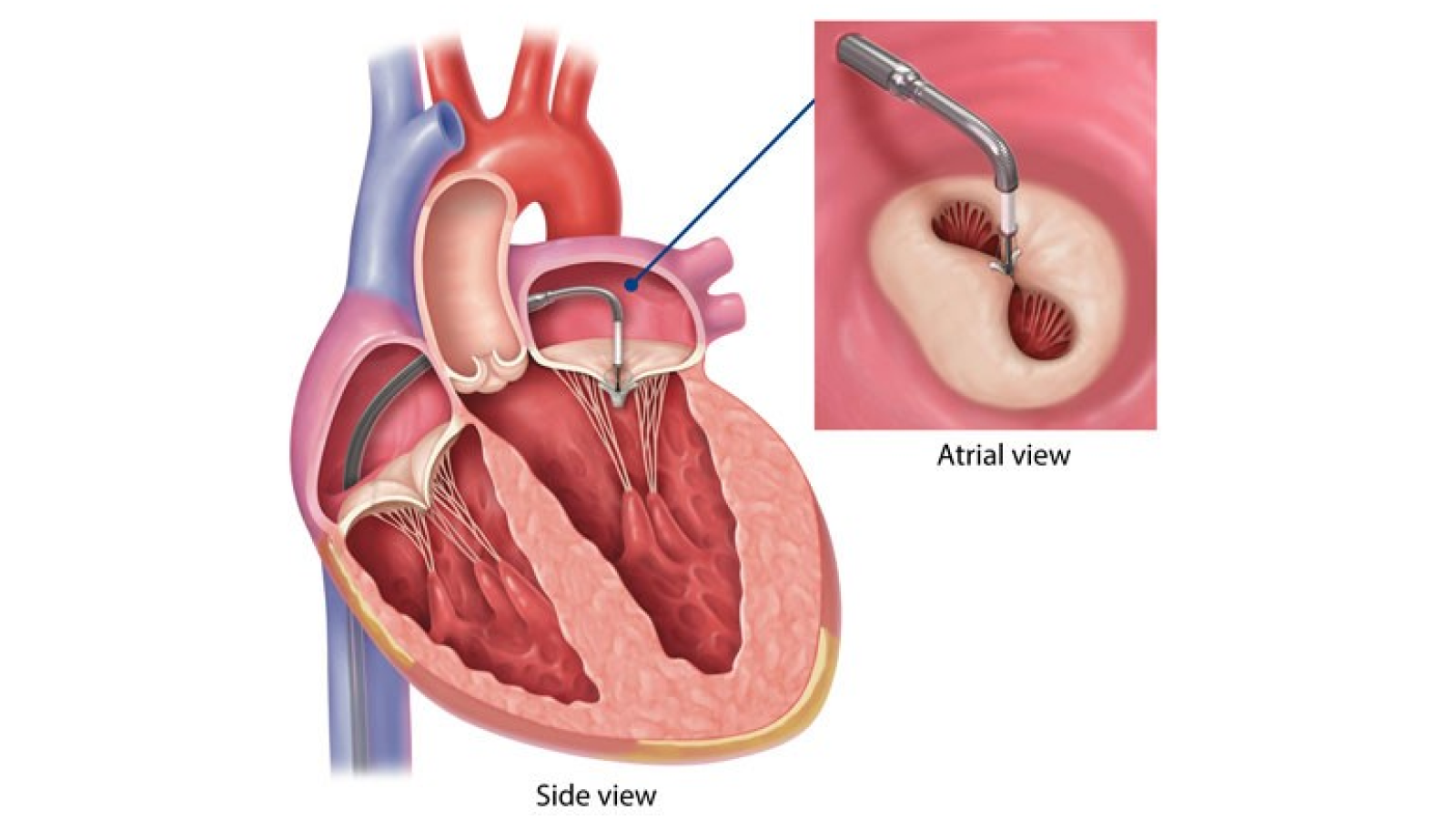
(i). Tricuspid Valve Repair/Replacement (TVR):
Tricuspid valve repair is a surgical procedure aimed at correcting problems with the right sided inlet valve leading to heart dysfunction. Surgical intervention for tricuspid valve repair is typically indicated when the valve dysfunction causes significant symptoms or cardiac dysfunction, and when medical therapy is insufficient. The primary goal of the surgery is to restore normal valve function, thereby improving cardiac efficiency and patient symptoms.
The surgical approach to tricuspid valve repair varies depending on the underlying pathology. Techniques include annuloplasty, where a ring is placed to tighten the valve annulus, and valve leaflet modification, where the valve leaflets are altered to improve coaptation. In more complex cases, the valve may need to be replaced with a bioprosthetic or mechanical valve.
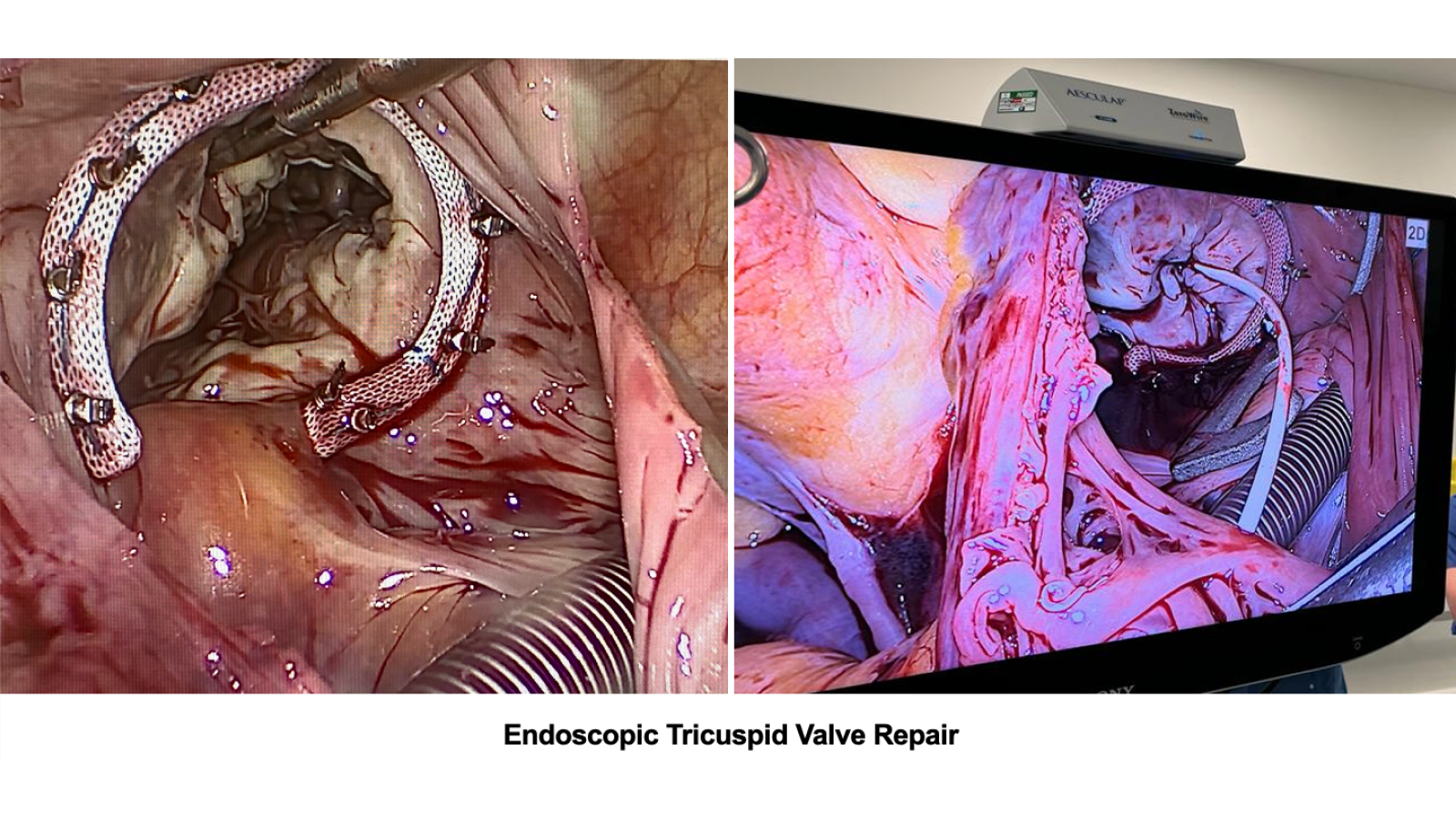
This surgery can be performed through traditional open-heart surgery, involving a sternotomy, or through less invasive methods like minimally invasive cardiac surgery (MICS), which involve smaller incisions and potentially reduced recovery times.
The risks of tricuspid valve repair surgery include bleeding, infection, arrhythmias, and valve dysfunction. However, when successfully performed, this surgery can significantly improve the quality of life and prognosis for patients with tricuspid valve disease. Postoperative care involves close monitoring, medication management, and cardiac rehabilitation to ensure optimal recovery and valve function.
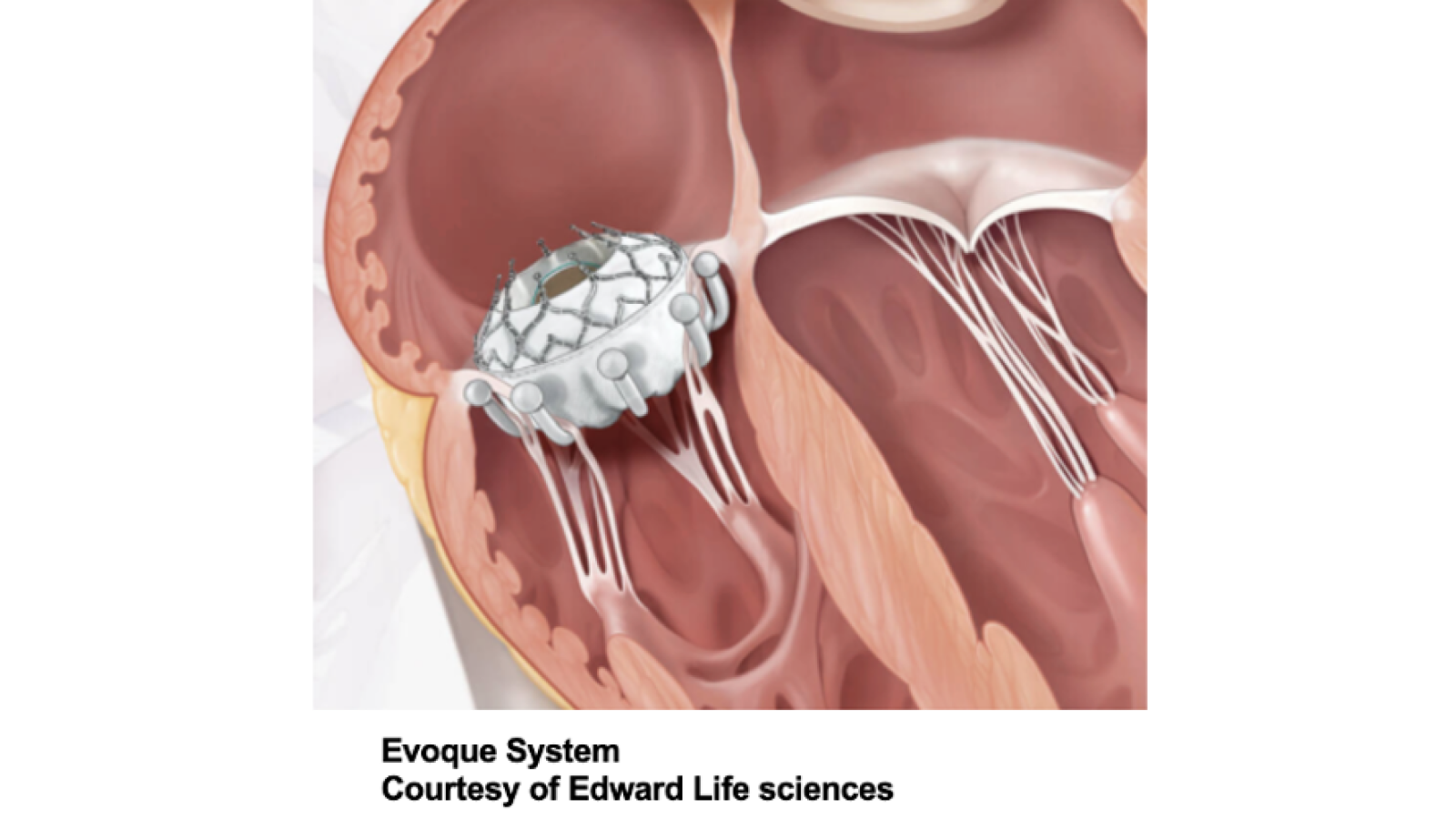
Transcatheter tricuspid valve repair and replacement represent an innovative advancement in cardiac surgery, especially for patients with tricuspid valve disease who are deemed high-risk for conventional surgery. Tricuspid regurgitation caused by tricuspid valve dysfunction causes, can lead to heart failure and other complications.
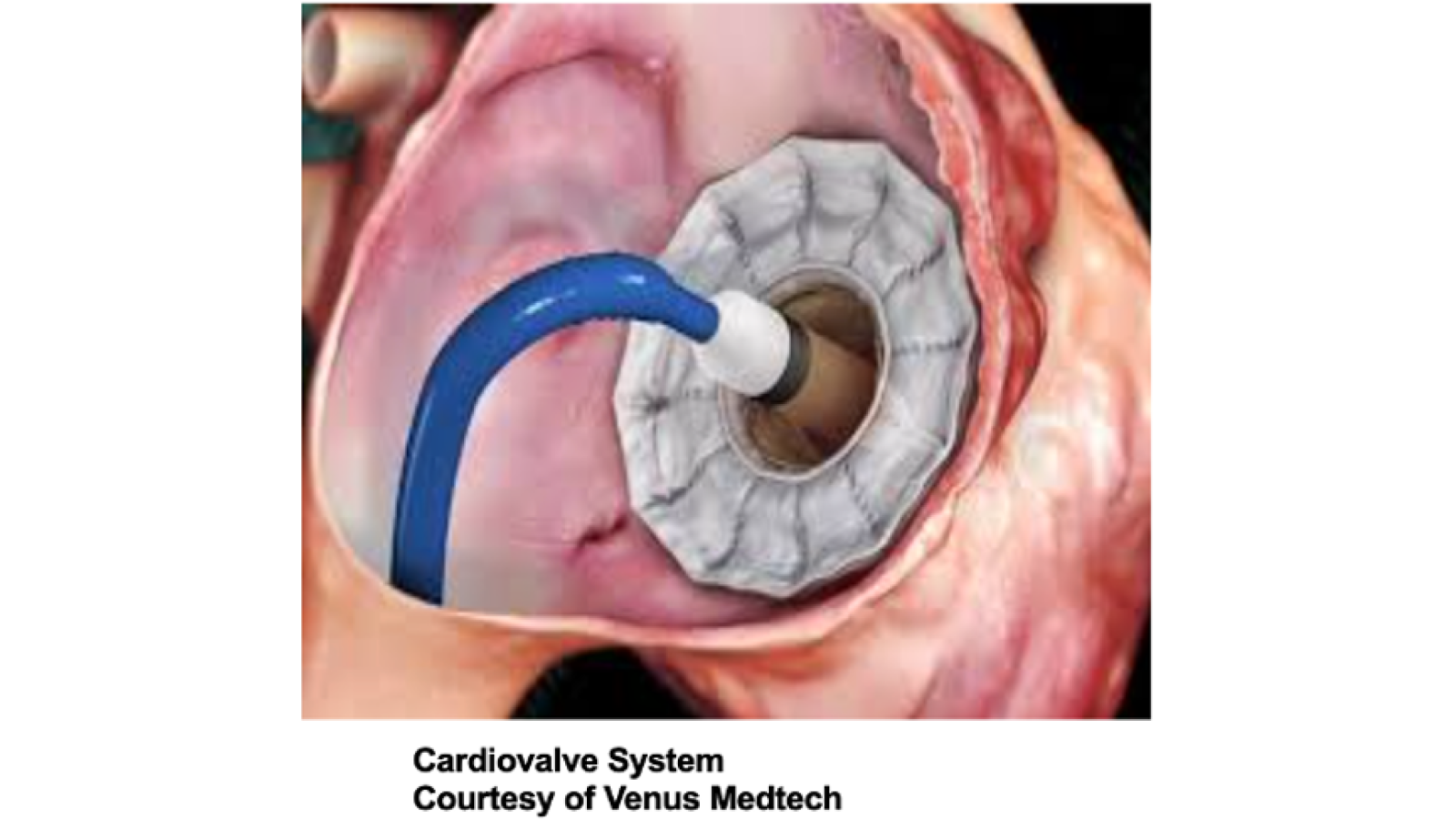
Transcatheter techniques involve the insertion of a catheter through a vein, usually in the groin, and navigate it to the heart. This approach significantly reduces the trauma and recovery time associated with traditional open-heart surgery. In transcatheter tricuspid valve repair, devices such as clips or bands are used to reshape the existing valve, improving its function. This method is particularly beneficial for patients whose condition may not necessitate full valve replacement or who are unable to undergo more invasive procedures.
Transcatheter tricuspid valve replacement, on the other hand, involves replacing the dysfunctional valve with a bioprosthetic one. This is done by collapsing the new valve into a small catheter, delivering it to the site, and then expanding it to replace the diseased valve. This procedure is typically reserved for cases where repair is not feasible or has failed.
Both techniques are guided by advanced imaging technologies, allowing for precise placement and deployment of devices. The use of echocardiography and fluoroscopy in real-time provides surgeons with detailed visual guidance throughout the procedure.
The benefits of transcatheter tricuspid valve interventions include reduced hospital stays, lower risk of infection, and quicker recovery
times. However, they also come with specific challenges and risks, such as the need for lifelong medication to prevent blood clots, potential damage to nearby cardiac structures, and the durability of the repair or replacement materials. Transcatheter approaches are continually evolving, with on-going research focusing on improving device design, expanding indications for use, and enhancing long-term outcomes.